September 25, 2014
Stanton A. Glantz, PhD
Best study on e-cigs for cessation so far shows they don't help and likely hurt
Sara Borderud and colleagues from Memorial Sloan Kettering Cancer Center just published an exceptionally well-done longitudinal study, "Electronic Cigarette Use Among Patients with Cancer,' on how use of e-cigarettes affects success in people trying to quit smoking as part of an organized smoking cessation program. It showed that, at best, the e-cigarette users did no better in quitting smoking and likely did a lot worse than smokers trying to quit who did not use e-cigarettes.
They assessed e-cigarette use among patients with cancer who had joined an evidence-based smoking cessation program at Sloan Kettering. The followed the patients for 6 to 12 months and assessed quitting success among people using e-cigarettes and those not using them.
In addition to being a prospective longtudinal study, other strengths include the fact that the investigators controlled for a range of demographic variables, the type of cancer the smokers had, and, most important, how addicted to nicotine they were (a common complaint about other studies from e-cigarette advocates).
The found that the e-cigarette users were more addicted on a variety of scales, but even after controlling for that, there was no difference in quitting at followup between people who did and did not use e-cigarettes.
Following standard procedure in doing such studies, the authors also did an intention to treat analysis in which the people lost to followup were treated as continuing smokers. This is likely the case because the e-cigarette users much more likely to drop out of the study [66% vs. 32% for nonusers) and reported having a harder time abstaning from smoking in smokefree environments than smokers who did not use e-cigarettes.) When the analysis was done this way smokers who used e-cigarettes were half as likely to quit smoking as smokers who did not use e-cigarettes. (The authors present them as twice as likely to still be smoking, which is the same thing.)
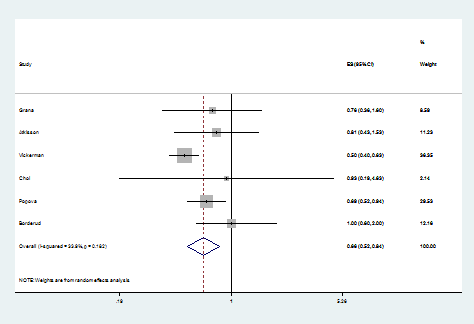
This result is consistent with the 5 other population-based studies in the meta-analysis we published in Circulation earlier this year, which found e-cigarette users were 39% less likely to quit smoking than smokers who did not use e-cigarettes. Adding this new study in the meta-analysis changes the numbers a bit, to a reduction in quitting of 34% if e-cigs don't affect quitting (top figure) and to a 42% drop based on the intention to treat analysis (bottom figure). (For statistics nerds, all 6 studies are still homogenous.)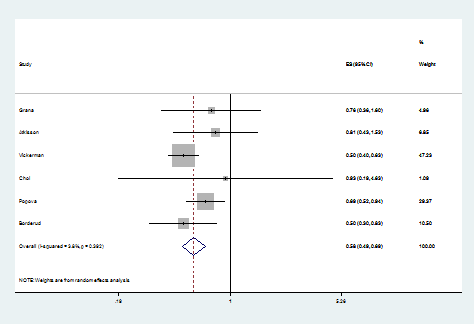
An experimental study by Andrea King and colleagues published in May 2014 helps explain this finding. They randomly exposed young adult smokers to people smoking conventional cigarettes and (separately) e-cigarettes. Both increased the urge to smoke conventional cigarettes.
This is the strongest evidence to date that health care providers should not be supporting the use of e-cigarettes for quitting and to advise smokers trying to quit to avoid dual use with e-cigarettes.
Here is the abstract:
BACKGROUND
Given that continued smoking after a cancer diagnosis increases the risk of adverse health outcomes, patients with cancer are strongly advised to quit. Despite a current lack of evidence regarding their safety and effectiveness as a cessation tool, electronic cigarettes (E-cigarettes) are becoming increasingly popular. To guide oncologists' communication with their patients about E-cigarette use, this article provides what to the authors' knowledge is the first published clinical data regarding E-cigarette use and cessation outcomes among patients with cancer.
METHODS
A total of 1074 participants included smokers (patients with cancer) who recently enrolled in a tobacco treatment program at a comprehensive cancer center. Standard demographic, tobacco use history, and follow-up cessation outcomes were assessed.
RESULTS
A 3-fold increase in E-cigarette use was observed from 2012 to 2013 (10.6% vs 38.5%). E-cigarette users were more nicotine dependent than nonusers, had more prior quit attempts, and were more likely to be diagnosed with thoracic and head or neck cancers. Using a complete case analysis, E-cigarette users were as likely to be smoking at the time of follow-up as nonusers (odds ratio, 1.0; 95% confidence interval, 0.5-1.7). Using an intention-to-treat analysis, E-cigarette users were twice as likely to be smoking at the time of follow-up as nonusers (odds ratio, 2.0; 95% confidence interval, 1.2-3.3).
CONCLUSIONS
The high rate of E-cigarette use observed is consistent with recent articles highlighting increased E-cigarette use in the general population. The current longitudinal findings raise doubts concerning the usefulness of E-cigarettes for facilitating smoking cessation among patients with cancer. Further research is needed to evaluate the safety and efficacy of E-cigarettes as a cessation treatment for patients with cancer. Cancer 2014. © 2014 American Cancer Society.
The paper, published in Cancer, is available here.
Comments
Can you respond to criticism of this study
Dear Prof Glantz, I saw criticism of this study in the news, I'd apreciate yo address it. (I feel both sides in this debate are not talking to each other enough):
http://in.reuters.com/article/2014/09/22/health-ecigarettes-cancer-idINK... target="_blank";http://in.reuters.com/article/2014/09/22/health-ecigarettes-cancer-idINK...
<blockquote;
"But Robert West, director of tobacco research at University College London, said the study was not able to assess whether or not for cancer patients who smoke using an e-cigarette to try and quit is beneficial "because the sample could consist of e-cigarette users who had already failed in a quit attempt, so all those who would have succeeded already would be ruled out".
Peter Hajek, director of the Tobacco Dependence Research Unit at Queen Mary, University of London, agreed that the study's data did not justify the conclusions.
"The authors followed up smokers who tried e-cigarettes but did not stop smoking, and excluded smokers who tried e-cigarettes and stopped smoking," he said.
"Like smokers who fail with any method, these were highly dependent smokers who found quitting difficult. The authors concluded that e-cigarette (use) was not helpful, but that would be true for any treatment however effective if only treatment failures were evaluated."
</blockquote;
West and Hajek do not appear to have read the paper carefully
Borderud and her colleagues took great pains to<em; account for exactly the potential problems that West and Hajek raise</em;. That is one of the reasons that I said it was the best study done to date.
The authors noted the number of prior quit attempts in their analysis and accounted explictly for level of addiction in their analysis.
Hajek's criticism is simply wrong. All smokers were followed up. The e-cigarette users were less likely to respond at follow-up, something the authors noted and accounted for in the intention to treat analysis, which is the same way that studies of conventional smoking cessation methods (like NRT) is done.
These are <em;strengths</em; not weaknesses of the study.
How do you adjust for resistance-to-treatment?
Can you make up for resistance-to-treatment by simply accounting for addiction?
Simply noting the number of prior quit attempts in the analysis is not fair; EC-related quit-attempts may be qualatively different.
Could this be related to the results??
http://www.carcinogenesis.com/article.asp?issn=1477-3163;year=2013;volum...
"Nicotine and its metabolites can promote tumor growth through increased proliferation, angiogenesis, migration, invasion, epithelial to mesenchymal transition, and stimulation of autocrine loops associated with tumor growth. Furthermore, nicotine can decrease the biologic effectiveness of conventional cancer treatments such as chemotherapy and radiotherapy."
David Bareham.
West and Hajek
I am not sure how to make the point any clearer - smokers who switched to EC and stopped smoking were not followed up, only those who continued to smoke were eligible for the study, This has nothing to do with controlling or not controlling for dependence. Suppose that cardiac bypass surgery removes angina pain in many patients but not in all. Now you select patients who had the surgery but it did not help with the pain (and there is no reason to expect any delayed effect). You follow them up and unsurprisingly, they have as much pain as patients who did not have the surgery. This would be a pretty pointless study and certainly not the best study there is to evaluate whether bypass surgery has any overall effect. Peter Hajek I e-mailed this reponse earlier but it was not included - I hope that it will make it this time. Cheers, Peter
This is a silly argument
Of course people who had previously quit smoking were not in the study.
You could make the same argument for people who quit cold turkey or with NRT.
Like all other cessaton studies if enrolled people who were trying o quit smoking at the time before the study started.
This is a silly argument
Of course people who had previously quit smoking were not in the study.
You could make the same argument for people who quit cold turkey or with NRT.
Like all other cessaton studies if enrolled people who were trying o quit smoking at the time before the study started.
West and Hajek
Not at all. This was not a cessation study, which would give smokers EC to see if it helps them to quit. It selected smokers who did not quit with EC and THEN followed them up. To use your analogy with NRT, if this study recruited people who were smoking after trying NRT, it would 'prove' that NRT does not help.
Different questions
I suppose that you are correct that this is not a <em;cessation trial </em;of e-cigarettes, which would require that patients be randomized to being provided e-cigrettes or not. That would be te relvant study if one were proposing to only make e-cigarettes available to people usig them as a cessaton aid by requiring prescription to purchase them.
That is not the reality, which is that anyone can buy them for ay purpose, in which case the apprpriate question (as thi study and all the other population-based studies except Brown/West did) is to ask how the use of e-cigarettes affects cessation success, which is overall a significant depressing in quittng.
The authors controlled for this
They measured nicotine addiction in several different ways, all of which were highly correlated.
High drop-out rate
Can you clarify the effects of the high drop-out rate has in the confidence of the results? From my understanding, drop-out rates of 10%-20% can introduce significant bias, and drop out rates of 66% would reduce the confidence of the results substantially. Treating the drop-outs as smokers is an assumption. Changing the assumption to an equally plausible one where the drop-outs were successful impacts the results substantially.
Also, by treating the drop-outs as smokers, the strongest statement you can make is "e-cigarettes help smokers quit AT LEAST x% of the time". This is a useful statement if you wanted to know the minimum rate of effectiveness, but not if you wanted to know what the actual rate of effectiveness is. A conservative assumption does not make the analysis better, it simply reduces the strength of the conclusion and provides information that is less useful. Comparing the minimum effectiveness of two treatments provides even less useful information.
The authors followed standard procedures
It would be nice if clincial trials and longitudinal studies could achieve 80%-90% retention, but, unfortunately, that is rarely the case.
The authors of this paper followed standard practice for smoking cessation studies by both evaluating their data as it was and by assuming people who dropped out continued to smoke (intention to treat). Experience has shown that such an appropach provides a reasonable estimate of what is actually going on. The dropouts were tended to be the more addicted smokers.
The results in this study are also consistent with most of the other large scale population studies that have been done, which show <em;less </em;quitting cigarettes among smokers who use e-cigarettes compared to smokers sho do not use e-cigarettes.
I have not doubt that <em;some </em;people have successfully quit using e-cigarettes. It is just theat e-cigarettes keep more people smoking. Whathttp://circ.ahajournals.org/content/129/19/e490.long" target="_blank"; I tell people is that if you want to try to quit smoking with e-cigarettes, you need to stop using cigarettes entirely while you are trying the e-cigarettes.
Add new comment